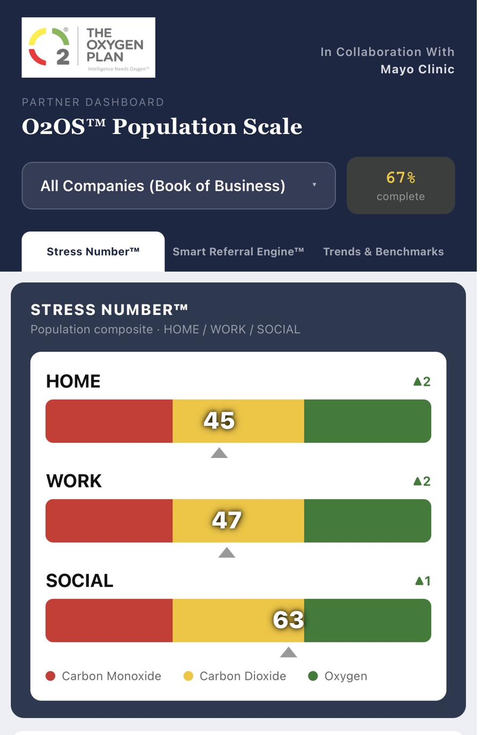
Stress Number™ — clinically validated Working in Collaboration with Mayo Clinic. Patent pending under USPTO Track One.
The federal payment system is converging on a single structural need at the same moment. The architecture built for that convergence was documented in 2008. It is architected as the reference coordinate for a federally activated market.

Four external clocks. One architecture filed in 2008.
O2OS™ is positioned at the intersection.
Reference-class infrastructure is what the federal payment system cites when it requires a credentialed standard.
The Oxygen Plan operates at that altitude.
Behavioral exposure is the largest unmeasured risk class on the institutional balance sheet.
Unmeasured risk is mispriced.
Mispriced risk creates structural cost.
The substrate now exists.
A coordinated behavioral accounting system — measurement, mapping, and routing primitives that compose into a single governable substrate.
Together, the three instruments constitute the behavioral accounting system that institutions, insurers, employers, providers, and AI systems will eventually coordinate around.
Patent Pending • Foundational behavioral risk telemetry architecture anchored to an 18-year documented record.
Every downstream system has been operating without a shared coordinate system for human behavioral exposure. Each absorbs the cost in its own currency — claims, PEPM, ordered diagnostics, unused telemetry, engagement loss, comp duration, downstream acuity, and tail risk. The same substrate sits upstream of all of it.
"Improving or Maintaining Mental Health" enters CMS Star Ratings at weight 1 in 2026 and rises to weight 3 beginning with the 2027 Star Ratings — equivalent to Diabetes Blood Sugar Control, Controlling Blood Pressure, and Plan All-Cause Readmissions. The federal payment system has just elevated behavioral measurement to a Medicare Advantage revenue lever.
The Pre-Diagnostic Index™ — derived from federal and peer-reviewed published sources, working in collaboration with Mayo Clinic, USPTO Track One patent-pending, with original patent application filed April 22, 2008 and published 2009 — is architected for this specification.
The Star Ratings move does not stand alone. The CMS ACCESS Model — outcome-aligned payments for behavioral health beginning July 2026 — and NCQA's 2026 directional priorities — Digital HEDIS expansion, ECDS measure growth, behavioral health integration — establish parallel federal directionality toward upstream behavioral measurement infrastructure. The corpus is aligned with all three.
Every prerequisite for institutional adoption is complete and on the public record.
The substrate is reimbursable, measurable, and federally aligned across six independent pathways. Each is a real federal designation. Each is publicly documented. Each is individually defensible.
| Pathway | What It Is |
|---|---|
| CMS CED | Medicare Coverage with Evidence Development — the pathway through which novel measurement standards gain Medicare coverage by providing prospective evidence to CMS. |
| CPT 96127 / 96138 | AMA Current Procedural Terminology codes for brief and standardized behavioral assessment — already reimbursable across commercial, Medicare, and Medicaid. |
| Medicaid 1115 Waivers | State waiver authority under Section 1115 of the Social Security Act — permits innovative Medicaid measurement, routing, and payment programs. |
| NCQA HEDIS | National Committee for Quality Assurance Healthcare Effectiveness Data and Information Set — the dominant national quality measure set for plan accreditation, including the DSF-E depression screening and follow-up measure. |
| CMS Star Ratings 2027 | Medicare Advantage "Improving or Maintaining Mental Health" — outcome measure, weight 3 beginning with the 2027 Star Ratings, equivalent in weight to Diabetes Blood Sugar Control and Controlling Blood Pressure. |
| CMS ACCESS Model | CMS Innovation Center Advancing Chronic Care with Effective, Scalable Solutions — outcome-aligned payment model for behavioral health, program begins July 5, 2026. |
CMS-0057-F creates the Pipe (real-time APIs), and the 2027 Star Ratings provide the Check (Quality Bonus Payments). O2OS™ is the Substrate that sits between the two — using the pipe to deliver the leading indicators that secure the check.
Access to the substrate is governed by a structured tier system. The structure is published rather than pitched. The model follows how standards bodies publish membership and licensing criteria — not how vendors run sales processes. Inquiries from qualified institutional counterparties are governed by the Inbound Response Protocol.
Inquiries: contact@theoxygenplan.com
Behavioral risk is unmeasured. Mispriced. Misrouted. Ungoverned.
The substrate that corrects all four now exists.
The substrate exists.
Institutional adoption and governance are the active formation phase.
O2OS™ is a behavioral measurement and coordination architecture developed over an 18-year period beginning in 2008.
Foundational disclosure dated to 2008 — authorship that predates the field.
US 2009/0265437 A1 — a publicly verifiable origin point preceding the mandates and infrastructure convergence now emerging across behavioral health.
Stress Number™ was clinically validated Working in Collaboration with Mayo Clinic and published in peer-reviewed research (Archives of Psychology, 2018; N=292).
A 2026 USPTO Track One application is now pending.
Products require adoption. Standards require recognition.
O2OS™ meets the foundational criteria of a clinical measurement reference standard — the formal designations are the roadmap ahead, not a present claim.