A coordination layer for human behavioral exposure has not previously existed at population scale. The corpus around it is now in active formation. This page documents the architecture, the institutional ecology, the structural dependency map, and the formation phase the corpus is entering.
The architecture predates the digital behavioral health era.
Filed April 22, 2008.
2009 PCT
Behavioral exposure is the largest unmeasured risk class on the institutional balance sheet. Across payers, employers, reinsurers, rating agencies, accreditation bodies, and sovereign systems, every actor that prices, governs, audits, or models behavioral exposure operates in a different language. The same underlying phenomenon — human behavioral state at population scale — is described through incompatible systems. None of them coordinate.
Approximately 95.8% of adults without a known behavioral health diagnosis receive no structured measurement of behavioral state — derived from CDC NCHS Data Brief No. 444 (2022) and the CMS Behavioral Health Strategy. They are not low-risk. They are unmeasured. Unmeasured risk is mispriced; mispriced risk creates structural cost; structural cost is now quantified.
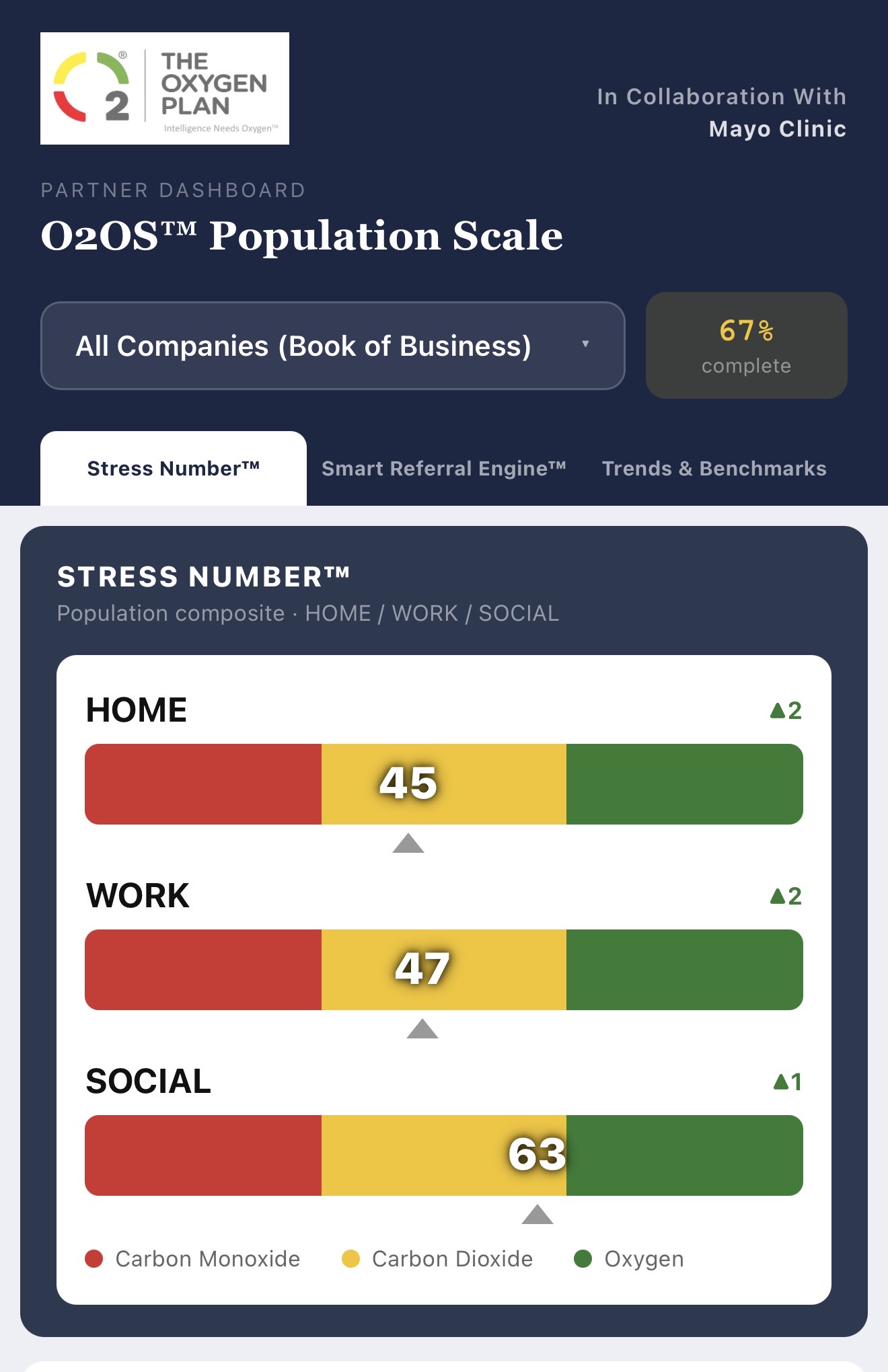
A pre-diagnostic measurement instrument has now been published, peer-reviewed working in collaboration with Mayo Clinic, federally aligned, and patent pending under USPTO Track One prioritized examination. The corpus around it constitutes the first credible candidate for a coordinate system that institutions can govern, price, and route against.
Two independent derivations converge within 7.3%.
NAMCS / NIMH / Greenberg pathway and CDC / PMC / AAFP pathway.
Public calculator at theoxygenplan.com/PDI.
Diagnostic instruments are not competitors. They are downstream tools that Stress Number™ routes individuals toward, when indicated. The category itself is different.
Pre-diagnostic is not a better diagnostic.
It is a different category, structurally upstream of clinical diagnosis.
The argument for the coordinate system is not rhetorical. Each step below is supported by the public record. Once the seven steps are admitted, the rational institutional response narrows.
FICO became the credit risk standard because lenders needed a unit to settle interstate transactions. CPT became the medical billing standard because Medicare needed a unit to reimburse procedures. HEDIS became the quality measurement standard because federal payment required outcome accountability. LOINC became the laboratory observation standard because interoperability required a shared code system. Each was a voluntary instrument that became effectively mandatory because the regulatory infrastructure converged on it. The Pre-Diagnostic Index™ now occupies that position for behavioral risk.
Eleven institutional classes are presently pricing, governing, auditing, routing, and modeling behavioral exposure — without a shared coordinate system. Their dependencies are structural, not commercial. The ecology below is a description of a market already in motion, operating against an absence the corpus now closes.
| Institutional Class | Why the Dependency Is Structural |
|---|---|
| Rating Agencies | Behavioral exposure is a material driver of medical loss ratio, workforce stability, and corporate operating risk. Agency models cannot rate accurately against a category that has no canonical measurement. |
| Reinsurers | Behavioral comorbidity is among the largest unpriced exposures in stop-loss, group life, disability, and long-tail medical treaties. Treaty pricing without a behavioral coordinate is structurally lossy. |
| National Payers | Behavioral exposure is the largest unmodeled cost driver. Payer captaincy of the substrate is the highest-leverage institutional position in the application layer. |
| Self-Insured Employers (Jumbo) | Aggregated behavioral exposure across self-insured populations exceeds the modeling capacity of any individual employer. Coordination requires a shared coordinate system. |
| Workers' Compensation Carriers | Behavioral comorbidity drives claim duration. Pre-diagnostic measurement at intake is the highest-leverage cost intervention point. |
| Big Four Governance Practices | Standards adoption, institutional measurement, and governance frameworks are the core deliverables. The behavioral category lacks the substrate against which the practice operates. |
| Accreditation Bodies | Quality measurement, certification, and audit functions require canonical instruments. The substrate becomes the reference standard those bodies certify against. |
| Sovereign Wealth Funds | Standards-class infrastructure produces non-linear durability, low marginal cost, and global dependence. Sovereign mandates favor perpetual coordination layers over operational businesses. |
| Assessment Publishers | Existing inventories (PHQ-9, GAD-7, HAM-D) are downstream clinical instruments. The pre-diagnostic substrate redefines what is measured and when. |
| AI & Clinical Decision Support | Agentic and adaptive systems making behavioral claims require standardized telemetry. The substrate is the regulatory and engineering anchor that downstream AI vendors will eventually require. |
| Sovereign Health Systems | National health coordination requires canonical pre-diagnostic measurement. The substrate is a candidate reference standard for population-scale behavioral risk pricing in single-payer systems. |
Eleven institutional classes presently absorb behavioral exposure as a structural absence. Once a coordinate system exists, the same classes gain new capabilities. The table below describes the capability emergence — not as a promise of adoption, but as the rational endpoint of the inevitability chain.
| Institutional Class | What Becomes Possible |
|---|---|
| Rating Agencies | Behavioral exposure becomes a measurable input. Rating models gain a coordinate where there was previously an unmodeled gap, allowing accurate differentiation across issuers and treaty pools. |
| Reinsurers | Treaty pricing gains a behavioral coordinate. Stop-loss, group life, and long-tail medical treaties can be structured against a normalized exposure metric rather than against an absence in the model. |
| National Payers | Behavioral exposure becomes a routable input upstream of utilization. Payer captaincy of the substrate establishes the highest-leverage position in the application layer. |
| Self-Insured Employers (Jumbo) | A shared coordinate system for behavioral exposure across populations becomes available, exceeding what any individual employer could construct. |
| Workers' Compensation Carriers | Claim duration gains a pre-diagnostic measurement point at intake — the highest-leverage cost intervention point in the comp lifecycle. |
| Big Four Governance Practices | Standards adoption, institutional measurement, and governance frameworks gain a substrate to operate from. The category gains a referenceable architecture rather than a vendor solution. |
| Accreditation Bodies | A canonical pre-diagnostic instrument exists to certify against. Quality measurement and audit functions gain a reference standard rather than constructing one. |
| Sovereign Wealth Funds | A standards-class coordination layer with non-linear durability and global reference dependence becomes available to allocate against. The asset class is infrastructure, not operations. |
| Assessment Publishers | Existing inventories (PHQ-9, GAD-7, HAM-D) gain an upstream architectural layer that redefines what is measured and when. Legacy instruments retain validity downstream of a coordinate system. |
| AI & Clinical Decision Support | Agentic and adaptive systems gain a standardized behavioral telemetry input — the regulatory and engineering anchor downstream AI systems will eventually require. |
| Sovereign Health Systems | A canonical pre-diagnostic measurement standard becomes available for population-scale behavioral risk pricing in single-payer systems. |
Conventional moats — distribution, network effects, switching costs — do not apply to substrate-class assets. Substrate moats operate through reference dependence: where dependent institutions reference a substrate in their audits, models, contracts, reimbursement workflows, compliance obligations, and AI training pipelines, replacement becomes systemically expensive in proportion to the breadth of dependency.
Standards reduce institutional transaction costs in measurable, compounding ways: decision latency in routing, reimbursement uncertainty in pricing, actuarial opacity in modeling, interoperability loss across institutional boundaries, and translation cost between counterparty languages. Every dependent institution captures friction reduction at the moment of reference.
GAAP, GPS, TCP/IP, CPT, and LOINC each became immortal not through marketing but through the asymmetric economics of friction reduction at coordination boundaries.
Compressing the friction that currently exists at every interface where one institution must reason about behavioral exposure originated by another — between payer and reinsurer, between employer and carrier, between rating agency and issuer, between AI system and clinical workflow.
None of these dependencies exist yet at scale. The structural argument is that they are the rational endpoint of the inevitability chain, not that they have already accreted.
Each deployment increases not only recurring revenue, but the intelligence density and defensibility of the coordination substrate itself.
Behavioral risk infrastructure follows a recognizable category-formation arc. The corpus is presently between Phase 2 and Phase 3. The phases that follow are not speculative — they are the standard maturation pattern observed in every prior infrastructure category, from accounting standards to credit ratings to clinical interoperability.
The architecture has been in formation since 2008. The 2026 USPTO Track One filing accelerates examination of work already published in 2009. The phases below describe the maturation arc — not the origination arc.
Verify U.S. Copyright Office registration TXu 1-576-009 →Phase 3 is the formative phase. It is the phase in which the substrate is operational and publicly documented, the institutional ecology is mapped, the governance architecture is articulated, and the counterparties who may define captaincy in their respective classes are first invited to engage. Phase 3 ends when institutional reference begins to accumulate.
The strategic position of an institution that engages during Phase 3 is structurally different from the position of an institution that engages in Phase 4 or Phase 5. Phase 3 entrants participate in the formation of the standard. Phase 4 entrants license the standard on terms set by Phase 3 captains. Phase 5 entrants reference the standard because it has become invisible infrastructure that cannot be operated without. The asymmetry compounds.
The institutional pathways for engaging with the corpus are structured, named, and tiered. They are described here for the same reason a regulator publishes a fee schedule: to make access conditions visible and stable. None of the structures below are sales offers — they are governance instruments through which the corpus organizes its institutional counterparties.
The O2OS™ governance architecture separates measurement infrastructure from care delivery, utilization incentives, and outcome-linked reimbursement structures. Revenue categories tied directly to routing, utilization management, or clinical outcome optimization are intentionally excluded from the core governance model in order to preserve measurement neutrality, interoperability credibility, and long-duration institutional trust.
The architecture is structured across four primary economic domains:
This separation is designed to support durable interoperability, cross-sector adoption, and independent institutional alignment.
Behavioral risk is unmeasured. Mispriced. Misrouted. Ungoverned.
The substrate that corrects all four now exists.
The substrate exists.
Institutional adoption and governance are the active formation phase.